
Understanding Endometriosis
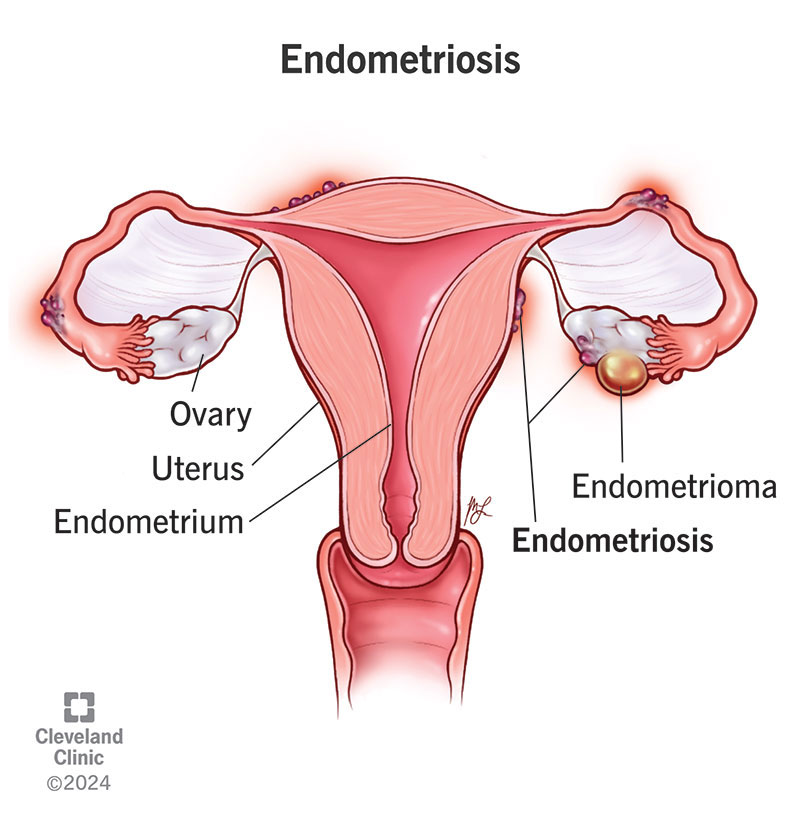
Endometriosis is a painful condition where tissue similar to the uterine lining (endometrium) grows outside the uterus. This abnormal growth results in chronic inflammation and complications such as adhesions, pelvic pain, and subfertility.
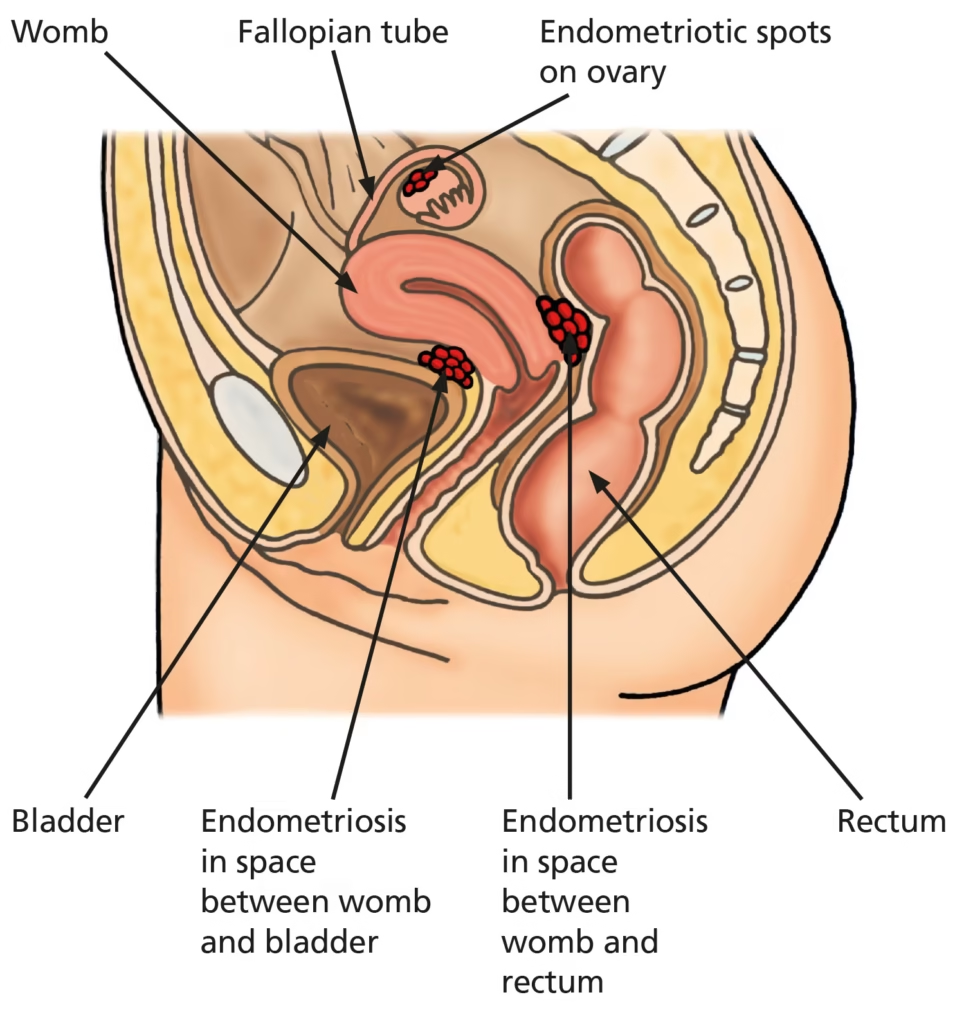
Endometriotic implants most commonly involve pelvic structures such as the ovaries, fallopian tubes, and peritoneum, but can also spread to the intestines, urinary tract, and structures outside the pelvic cavity.
Globally, endometriosis affects approximately 1 in 10 women, making it a relatively common gynecological condition. It’s more prevalent in women who experience painful periods (dysmenorrhea) and those dealing with subfertility.
This might help: TCM for Period Cramps in Singapore: How it Works
Types of Endometriosis
Endometriosis can be classified into three distinct types based on the location where the endometrial tissue develops outside the uterus.
Superficial Peritoneal Lesion represents the most common type of endometriosis, where lesions develop on the peritoneum, which is the thin film that lines the pelvic cavity.
This form typically involves small patches of endometrial tissue that implant on the surface of pelvic organs and structures.
Endometrioma or Endometriotic Cyst, also known as ovarian lesions, develops specifically within the ovaries.
These cysts are often called “chocolate cysts” due to the characteristic dark brown fluid inside that resembles chocolate syrup in appearance.
This fluid consists of old menstrual blood and endometrial tissue that has accumulated over time within the ovarian cyst.
Deeply Infiltrating Endometriosis (DIE) represents the most severe form, developing below the peritoneum where it can penetrate deeply into surrounding tissues.
This type can affect nearby organs such as the bladder and bowels, causing significant complications and symptoms.
Deeply infiltrating endometriosis affects approximately 1% of women of reproductive age, making it the least common but most serious form of the condition.
Related article: TCM for Irregular Menstruation
Signs and Symptoms
Many women with endometriosis experience one or more characteristic symptoms that can significantly impact their quality of life.
Painful periods, known medically as dysmenorrhea, occur as endometriosis tissue breaks down and leads to bleeding inside the pelvis, resulting in inflammation, swelling, and intense pain that often exceeds normal menstrual discomfort.
Pain during intercourse, called dyspareunia, develops due to physical interaction between the penis and the enlarged uterus and pelvic endometriosis lesions during sexual activity.
Many women also experience pain during urination or bowel movements, especially during menstrual periods when the endometrial tissue is most active and inflamed.
You might want to read: Irritable Bowel Syndrome (IBS): Causes, Symptoms and Treatment in Singapore
Menstrual irregularities are common and include heavy menstrual bleeding, particularly in cases of adenomyosis where endometriosis affects the muscle layer of the uterus.
Prolonged menstrual bleeding often occurs due to the thickened endometrium taking longer to shed completely.
Some women experience bleeding between periods, manifesting as irregular spotting or breakthrough bleeding that can be unpredictable and concerning.
Infertility represents one of the most serious complications of endometriosis, occurring when the condition damages fallopian tubes and blocks the normal pathway for egg and sperm fertilization.
Long-term lower back and pelvic pain develop due to chronic inflammation and the formation of pelvic adhesions that can bind organs together.
Additional symptoms can include persistent fatigue, abdominal bloating, nausea, and digestive issues such as diarrhea or constipation during menstrual periods.
However, it’s important to note that some women with endometriosis experience no symptoms at all and may only discover the condition during an infertility evaluation or routine gynecological examination.
Read more: Which Gynaecologist in Singapore Should You Consider?
Risk Factors
Several factors may increase the risk of developing endometriosis, though having these risk factors doesn’t guarantee that a woman will develop the condition.
Family history plays a significant role, as having a relative with endometriosis increases the likelihood of developing the condition, suggesting a genetic component to the disease.
Never having been pregnant appears to increase risk, possibly because pregnancy and breastfeeding reduce the total number of menstrual cycles a woman experiences throughout her reproductive years.
Medical conditions that affect normal menstrual flow, such as structural abnormalities of the uterus, can also increase the risk by altering how menstrual blood flows out of the body.
Hormonal factors influence risk as well.
Earlier onset of menstruation or later menopause exposes women to more menstrual cycles throughout their lifetime, potentially increasing the risk of endometrial tissue implanting outside the uterus.
Similarly, shorter menstrual cycles or heavier menstrual periods may increase the likelihood of retrograde menstruation, where menstrual blood flows backward through the fallopian tubes into the pelvic cavity.
You might be interested: Understanding Low Libido in Women: Causes, Treatment and Impact
 Biofinest Effervescent Vitamin C 1000mg D3 Zinc Collagen Multivitamin Calcium Magnesium Zinc Tablets Drink Sugar FreeFrom $5.25 $11.93Check Price on Shopee【 SG Stock 】All-In-One Multi Pouch Shake / Macadamia, Cinnamon, Chocolate / Protein, Korea Diet meal$9.90Check Price on Shopee-95%Estalife Daily Pre + Probiotics Melts + Enzyme | 15 Billion CFU + Inulin + Bromelain | 肠道保健From $1.99 $39.80Check Price on Shopee-70%Estalife Magnesium Glycinate 1000MG | Heart, Bone, Muscle, Sleep, Mood Health | 60 Veg CapsFrom $13.43 $44.77Check Price on Shopee-78%Biofinest Probiotic 50 Billion CFU Enzyme Supplement 12 + 3 Prebiotics – Diet Slimming Eczema Detox Men Women (60 caps)From $22.00 $100.00Check Price on Shopee-31%Optimum Nutrition, Gold Standard, 100% Whey Protein Powder, 2lbs (907g ) / 5 lbs (2.27 kg) / 10 lbs (4.54 kg)From $40.35 $58.48Check Price on Shopee-56%Optimum Nutrition, Micronized Creatine Powder, Build Muscle, Workout Support, Unflavored, 300g-1200gFrom $34.50 $78.41Check Price on Shopee-12%Shortcutx Max Fat Burner Juice • Made in UK • Weight Loss Supplement for Slimming • Clinically proven (7 sachets)From $34.31 $38.99Check Price on Shopee
Biofinest Effervescent Vitamin C 1000mg D3 Zinc Collagen Multivitamin Calcium Magnesium Zinc Tablets Drink Sugar FreeFrom $5.25 $11.93Check Price on Shopee【 SG Stock 】All-In-One Multi Pouch Shake / Macadamia, Cinnamon, Chocolate / Protein, Korea Diet meal$9.90Check Price on Shopee-95%Estalife Daily Pre + Probiotics Melts + Enzyme | 15 Billion CFU + Inulin + Bromelain | 肠道保健From $1.99 $39.80Check Price on Shopee-70%Estalife Magnesium Glycinate 1000MG | Heart, Bone, Muscle, Sleep, Mood Health | 60 Veg CapsFrom $13.43 $44.77Check Price on Shopee-78%Biofinest Probiotic 50 Billion CFU Enzyme Supplement 12 + 3 Prebiotics – Diet Slimming Eczema Detox Men Women (60 caps)From $22.00 $100.00Check Price on Shopee-31%Optimum Nutrition, Gold Standard, 100% Whey Protein Powder, 2lbs (907g ) / 5 lbs (2.27 kg) / 10 lbs (4.54 kg)From $40.35 $58.48Check Price on Shopee-56%Optimum Nutrition, Micronized Creatine Powder, Build Muscle, Workout Support, Unflavored, 300g-1200gFrom $34.50 $78.41Check Price on Shopee-12%Shortcutx Max Fat Burner Juice • Made in UK • Weight Loss Supplement for Slimming • Clinically proven (7 sachets)From $34.31 $38.99Check Price on ShopeeDiagnosing Endometriosis in Singapore
Diagnosing endometriosis typically involves a systematic approach using several diagnostic methods to accurately identify and assess the extent of the condition.
The process begins with a comprehensive medical history and physical examination, where your doctor will ask detailed questions about your symptoms, including their timing, severity, and relationship to your menstrual cycle.
A physical examination may include a pelvic exam to check for endometriotic cysts and scar tissue that can be felt during the examination.
Imaging tests provide valuable information about the presence and location of endometriosis lesions. Ultrasound scanning can effectively identify endometriotic ovarian cysts and assess their size and characteristics.
Magnetic Resonance Imaging (MRI) offers more detailed visualization and can detect endometriosis lesions within the walls of the uterus and other pelvic structures that may not be visible on ultrasound.
Laparoscopy remains the only definitive way to confirm endometriosis diagnosis with absolute certainty.
This minimally invasive surgical procedure involves inserting a thin tube with a camera, called a laparoscope, through a small incision in the abdomen.
This technique allows direct visual inspection of the pelvic organs and enables the surgeon to identify endometriosis lesions, take tissue biopsies for microscopic examination, and determine the severity of endometriosis through standardized staging systems.
Healthcare providers may also use validated endometriosis questionnaires to assess whether painful menstruation and associated symptoms indicate the likelihood of endometriosis.
These standardized tools help doctors evaluate symptom patterns and determine which patients would benefit most from further diagnostic testing.
Related article: HPV Vaccination in Singapore: A Comprehensive Guide
Treatment Options for Endometriosis in Singapore
Treatment approaches for endometriosis are highly individualized and depend on several important factors that help guide therapeutic decisions.
The severity of symptoms experienced by the patient plays a crucial role in determining the most appropriate treatment approach, as women with mild symptoms may require different interventions than those with severe, debilitating pain.
The extent of endometriosis, as determined through diagnostic procedures, significantly influences treatment planning.
Minimal endometriosis may respond well to conservative treatments, while extensive disease involving multiple organs may require more aggressive surgical intervention.
Patient age is another important consideration, as younger women may prioritize fertility preservation while older women nearing menopause might choose different treatment strategies.
Perhaps most importantly, whether a woman hopes to become pregnant in the near future fundamentally shapes treatment decisions, as some therapies that effectively control symptoms may temporarily or permanently affect fertility.
These factors work together to help healthcare providers and patients develop personalized treatment plans that address individual needs, preferences, and life circumstances while providing optimal symptom relief and preserving reproductive potential when desired.
You might like: Menopause Treatment Singapore
Non-Medical Approaches
- Lifestyle modifications
- Regular exercise
- Healthy diet low in gluten and processed foods
- Stress management techniques
Pain Management
- Over-the-counter pain relievers
- Non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen
- Paracetamol (Panadol)
- Specialized pain management
- Referral to chronic pain clinics in severe cases
Hormonal Therapy
Hormonal treatments aim to slow down the growth and progression of endometriosis by regulating the hormones responsible for its growth. Options include:
- Oral contraceptive pills
- Regulates menstrual cycles
- Reduces pain and inflammation
- Progestins (such as dienogest)
- Reduces endometriosis activity
- Available in pill form or as injections
- Gonadotropin-releasing hormone (GnRH) medicines
- Reduces estrogen production
- Creates a temporary menopause-like state
- Androgenic hormones
- Reduces effects of estrogen on endometriosis
- Aromatase inhibitors
- Newer therapy option for some cases
Read more: Hysterectomy in Singapore: Costs, Risks, Treatment
Important Considerations for Hormonal Therapy
Hormonal therapy for endometriosis requires careful consideration of several important factors that affect treatment effectiveness and patient outcomes.
These medications typically need to be taken long-term to maintain symptom control, as endometriosis is a chronic condition that tends to persist throughout a woman’s reproductive years.
The commitment to long-term treatment means that patients must be prepared for ongoing medication management and regular monitoring by their healthcare providers.
Stopping hormonal treatment often leads to recurrence of symptoms, as the underlying endometriosis tissue remains active and responsive to natural hormonal fluctuations.
This means that women who discontinue therapy may experience a return of pain, heavy bleeding, and other symptoms within a relatively short time after stopping medication.
It’s crucial to understand that hormonal therapy does not remove existing endometriosis lesions or cure the condition.
Instead, these medications work by suppressing the growth and activity of endometrial tissue, providing symptom relief while the tissue remains in place.
This limitation means that hormonal therapy is primarily a management strategy rather than a definitive treatment.
In some cases, additional treatments such as surgery may be needed even while using hormonal therapy, particularly when large cysts develop or when symptoms are not adequately controlled by medication alone.
Finally, hormonal therapy is not suitable for women who are actively trying to conceive, as most hormonal treatments suppress ovulation and prevent pregnancy while being used.
Surgical Treatment
Surgery becomes a viable and often necessary treatment option when conservative medical management fails to provide adequate symptom relief or when specific clinical circumstances warrant intervention.
Medical treatments may fail to control symptoms effectively in cases of severe or extensive endometriosis, leaving surgery as the next appropriate step in the treatment pathway.
Surgery is particularly indicated when pain becomes severe and significantly impacts a woman’s quality of life, work performance, and daily activities despite optimal medical management.
The presence of large endometriotic cysts, especially those that may be causing complications or interfering with normal organ function, often requires surgical removal to prevent further problems and provide symptom relief.
Fertility considerations frequently drive surgical decision-making, as endometriosis can significantly affect a woman’s ability to conceive naturally.
When fertility is compromised by endometriosis lesions, adhesions, or ovarian cysts, surgical intervention may be necessary to restore normal anatomy and improve the chances of successful conception.
Surgery can remove endometriosis lesions, separate adhesions that may be distorting pelvic anatomy, and restore normal ovarian and tubal function when possible.
Types of surgical approaches:

- Laparoscopic surgery (minimally invasive)
- Small incisions allow insertion of a camera and surgical instruments
- Endometriotic lesions and cysts can be removed
- Recovery time: approximately two weeks
- Preferred approach for most cases
- Laparotomy (open surgery)
- Larger incision across the lower abdomen
- Used for more severe or complex cases
- Recovery time: up to one month
- Higher risk of complications
- Specialized surgical techniques
- Robotic keyhole surgery for severe cases offers more precision
- Should be performed by specialists in endometriosis surgery
- Hysterectomy (removal of uterus)
- With or without removal of ovaries
- Last resort treatment for severe cases
- Only considered when:
- Other treatments have failed
- Pain is debilitating
- The woman has completed her family
- Important note: A woman cannot get pregnant after hysterectomy
Fertility Treatments
For women with endometriosis experiencing infertility:
- Surgery to improve natural conception
- Removing endometriosis deposits or endometriotic ovarian cysts
- Most effective for minimal to moderate endometriosis
- Majority of pregnancies occur within six months after surgery
- Assisted reproductive techniques
- Intrauterine insemination (IUI) with fertility drugs
- For minimal to moderate cases
- In vitro fertilization (IVF)
- Fertilization of mature eggs with sperm in a laboratory
- May be the first choice for severe endometriosis to avoid surgical complications
- Studies suggest IVF success rates improve after surgical treatment of endometriosis
- Intrauterine insemination (IUI) with fertility drugs
Multidisciplinary Care
Comprehensive management of endometriosis often requires a coordinated team approach involving multiple medical specialists, as the condition can affect various organ systems and aspects of a woman’s health.
This collaborative approach ensures that all aspects of the disease are addressed appropriately and that patients receive the most comprehensive care possible.
Gynecologists who specialize in endometriosis and minimally invasive surgery form the cornerstone of the treatment team, providing expertise in diagnosing the condition, performing complex surgical procedures, and managing the gynecological aspects of the disease.
These specialists understand the nuances of endometriosis surgery and can perform procedures that preserve fertility while effectively removing disease.
Fertility specialists become essential team members when endometriosis affects a woman’s ability to conceive, offering specialized treatments such as in vitro fertilization (IVF) and other assisted reproductive technologies.
Their expertise in reproductive medicine helps optimize pregnancy outcomes for women with endometriosis-related infertility.
When endometriosis involves the bowel, bowel specialists or colorectal surgeons may be needed to safely manage lesions affecting the intestinal tract while preserving normal bowel function.
Similarly, bladder specialists or urologists may be required when the urinary tract is involved, ensuring that treatments address urinary symptoms without compromising kidney or bladder function.
Pain management specialists play a crucial role in helping women cope with chronic pain associated with endometriosis, offering various approaches including medication management, nerve blocks, and other interventional techniques.
Their expertise is particularly valuable for women with persistent pain that doesn’t respond completely to hormonal or surgical treatments.
Psychological and psychosexual support represents an often-overlooked but vitally important component of comprehensive endometriosis care.
The chronic nature of the condition, its impact on sexual function, and the stress of dealing with infertility can significantly affect mental health and relationships.
Professional counseling and support help women develop coping strategies, address relationship challenges, and maintain emotional well-being throughout their treatment journey.
Preparing for Endometriosis Surgery
If surgery is recommended, preparation is key:
- Support system
- Arrange for a friend or family member to accompany you
- Pre-operative instructions
- Follow fasting guidelines (specific instructions will be provided)
- Inform your doctor about any medications you’re taking
- Stop smoking
- Recovery planning
- Arrange time off work
- Prepare your home for recovery
- Understand post-operative care instructions
Post-Surgical Recovery
Recovery timeframes vary based on the type of surgery:
- After laparoscopy
- Typically discharged the same day
- Return to normal activities within two weeks
- Follow-up appointments are crucial
- After laparotomy
- Hospital stay may be required
- Full recovery may take up to one month
- More extensive rest period needed
Managing Endometriosis Long-Term
Since endometriosis tends to recur, long-term management strategies include:
- Continued medical therapy
- Hormonal treatments may be recommended after surgery
- Regular follow-ups with your gynecologist
- Family planning considerations
- Women who plan to conceive are advised to do so as soon as possible after endometriosis surgery
- Discuss fertility preservation options if pregnancy isn’t immediately planned
- Psychological support
- Endometriosis can impact mental health and relationships
- Support groups and counseling may be beneficial
The Impact of Endometriosis on Quality of Life
Endometriosis can be a physically and mentally debilitating disease affecting every aspect of a woman’s life.
Women with endometriosis tend to have more difficulties maintaining careers and relationships due to chronic pain and fertility issues.
Seeing a gynecologist who specializes in this area and has access to supporting clinics in other specialties provides the best opportunity to keep the pain under control and achieve fertility goals.
FAQ
What is the prevalence of endometriosis?
Globally, it is estimated that 1 in 10 women are affected by endometriosis.
It is more common in women with dysmenorrhea (painful periods) and subfertility. Despite being relatively common, many cases remain undiagnosed or are diagnosed after years of symptoms.
Can endometriosis be cured?
Currently, there is no definitive cure for endometriosis. Treatment approaches focus on managing symptoms, slowing disease progression, and addressing fertility concerns.
Surgical removal of endometriotic lesions can provide temporary relief, but the condition may recur over time.
Long-term management typically involves a combination of medical treatments and lifestyle modifications.
How does endometriosis affect fertility?
Endometriosis is one of the major causes of female infertility. It can impact fertility through several mechanisms: damaging fallopian tubes, creating a hostile environment for embryo implantation, affecting egg quality, or causing hormonal imbalances.
However, many women with endometriosis do successfully conceive, either naturally or with fertility treatments.
The severity of endometriosis doesn’t always correlate with fertility impact—some women with severe endometriosis conceive without difficulty, while others with mild disease may experience fertility challenges.
What are the complications of endometriosis?
Complications of endometriosis include infertility, damage to surrounding tissues such as the bladder and bowel, formation of adhesions (bands of scar tissue that can bind organs together), chronic pain that affects quality of life, and psychological impacts such as depression and anxiety. In rare cases, endometriosis implants can invade other organs and cause functional problems.
Additionally, women with endometriosis have a slightly elevated risk of developing certain types of ovarian cancer, though this risk remains low overall.
Is endometriosis hereditary?
There appears to be a genetic component to endometriosis. Women who have a first-degree relative (mother, sister, or daughter) with endometriosis have approximately 7-10 times higher risk of developing the condition themselves.
However, genetics is likely only one factor among many contributing to endometriosis development.
Environmental factors, immune system function, and hormonal influences also play important roles in determining who develops this condition.
How is endometriosis different from adenomyosis?
While both conditions involve endometrial-like tissue growing in abnormal locations, they are distinct conditions.
Endometriosis occurs when endometrial-like tissue grows outside the uterus—on the ovaries, fallopian tubes, or other pelvic structures. Adenomyosis, however, involves endometrial tissue growing into the muscular wall of the uterus itself.
Both conditions can cause painful periods and heavy bleeding, but adenomyosis specifically leads to an enlarged, tender uterus.
Treatment approaches may differ between the two conditions, though some therapies like hormonal treatments can help with both.
What should I expect during a laparoscopy for endometriosis?
During a laparoscopic procedure for endometriosis, you’ll be under general anesthesia.
The surgeon will make small incisions (usually 0.5-1 cm) in your abdomen, typically one in the navel and 2-3 others in the lower abdomen.
A laparoscope (thin tube with a camera) will be inserted to visualize the pelvic organs, and specialized instruments will be used to remove or destroy endometriotic lesions and adhesions.
The procedure typically takes 1-3 hours depending on the extent of the disease. Most patients go home the same day, though overnight observation may be needed in complex cases.
Recovery generally takes 1-2 weeks, with some restrictions on physical activity during that time.
How effective are hormonal treatments for endometriosis?
Hormonal treatments are effective for many women in managing endometriosis symptoms, particularly pain.
Success rates vary depending on the specific medication and individual factors.
For example, combined oral contraceptives reduce pain in approximately 70-80% of women, while GnRH agonists may provide relief for up to 90% of women.
However, hormonal treatments do not remove existing endometriosis; they work by suppressing new growth and reducing inflammation.
Symptoms typically return when treatment is discontinued. Additionally, side effects vary between different hormonal options and need to be considered when choosing a treatment approach.
Can endometriosis affect organs outside the pelvic area?
While endometriosis most commonly affects pelvic structures, it can occasionally be found in locations outside the pelvic cavity.
In rare cases, endometriotic tissue has been discovered in the lungs, diaphragm, abdominal wall, and even the brain.
These distant sites can cause unusual symptoms that may not immediately suggest endometriosis, such as cyclical shoulder pain, chest pain, or coughing blood during menstruation (in cases of thoracic endometriosis).
Diagnosis of extra-pelvic endometriosis often requires specialized imaging and a high index of suspicion from healthcare providers.
How does Singapore’s healthcare system support endometriosis patients?
Singapore’s healthcare system provides comprehensive support for endometriosis patients through both public and private healthcare facilities.
Specialized gynecologists trained in minimally invasive surgery are available at major hospitals.
The healthcare system facilitates multidisciplinary care, allowing collaboration between gynecologists, fertility specialists, pain management experts, and mental health professionals.
Some institutions have dedicated endometriosis clinics or centers providing coordinated care.
Singapore’s advanced medical technology enables precise diagnosis and treatment through high-resolution imaging and advanced surgical techniques.
While costs vary between public and private sectors, government subsidies, MediSave, and insurance coverage help make treatments more affordable for eligible patients.
Optimum Nutrition Gold Standard 100% Whey Protein, 5 LBs | Double Rich Chocolate | Primary Source Isolate$132.43 $139.40Check Price on Shopee-56%Biofinest Gummy Vitamin Supplement – Beauty Energy Sleep Metabolism Men Women Kids Probiotics Multivitamin (60 Gummies)From $17.55 $39.89Check Price on Shopee-65%PM12 Balporo Bbae 1Box [Slimming, Weight Loss supplement, Garcinia,Vitamin, Effervescent]From $12.39 $35.40Check Price on Shopee-13%Tradishot Detox Juice • Traditional Modern Tasty Jamu • Natural Herbal Supplement • Tumeric shot [7 x 35ml]From $24.36 $28.00Check Price on Shopee-12%[NEW] Shortcutx Max+ Advanced Fat Burner Juice • Improved Formula For Extreme Weight Loss (15x35ml)$71.95 $81.76Check Price on Shopee-18%Tradishot Immunity Boost Drink | Turmeric Shot (Extra Strength) | Boost Immunity Energy & Well-being [7x35mL]$24.60 $30.00Check Price on Shopee-30%Biofinest Omega 3 Fish Oil 1000mg – Wild Alaskan Fish Natural Vitamin E Omega 3 EPA DHA – Heart Brain (300 Softgels)$26.35 $37.64Check Price on Shopee-76%I Love Smart Heart Goat Pet Milk 70ml 400ml for Cats and DogsFrom $1.19 $4.96Check Price on Shopee