
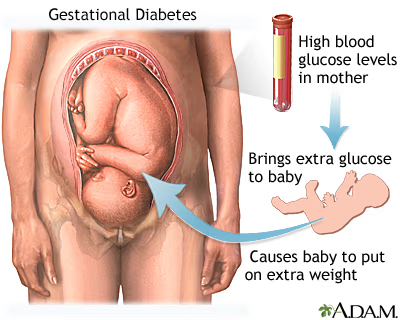
Gestational diabetes mellitus (GDM) is a condition that develops during pregnancy when the mother’s body cannot produce sufficient insulin or cannot use insulin effectively due to natural bodily changes occurring during pregnancy.
In Singapore, this condition affects approximately 1 in 5 pregnant women, making it a common pregnancy complication that requires proper understanding and management.
Understanding Gestational Diabetes
Gestational diabetes typically emerges in the second or third trimester of pregnancy, commonly between the 24th and 28th week.
During pregnancy, hormonal changes can cause the body to become resistant to insulin, the hormone responsible for regulating blood sugar levels.
While the pancreas normally produces extra insulin to overcome this resistance, GDM occurs when the body cannot produce enough insulin to meet the increased demands during pregnancy.
Read more: Which Endocrinologist in Singapore Should You Consider?
The exact science behind why some women develop GDM while others do not is not fully understood.
However, it’s important to understand how pregnancy affects glucose regulation in your body.
Normally, glucose from food is absorbed into the bloodstream, and insulin allows your body to use or store this glucose.
During pregnancy, the production of various hormones can reduce insulin effectiveness, potentially leading to unregulated blood sugar levels that may affect both mother and baby.
 OMY Liquid Hyaluron 2.0 | Marine Collagen 28,000mg + PDRN 1,000mg | Hydrating Bouncy Skin Glow Drink$70.00Check Price on Shopee-55%Biofinest Effervescent Vitamin C 1000mg D3 Zinc Collagen Multivitamin Calcium Magnesium Zinc Tablets Drink Sugar FreeFrom $5.35 $11.89Check Price on Shopee【 SG Stock 】All-In-One Multi Pouch Shake / Macadamia, Cinnamon, Chocolate / Protein, Korea Diet meal$9.90Check Price on Shopee-60%Estalife Daily Pre + Probiotics Melts + Enzyme | 15 Billion CFU + Inulin + Bromelain | 肠道保健From $19.99 $49.98Check Price on Shopee-70%Estalife Magnesium Glycinate 1000MG | Heart, Bone, Muscle, Sleep, Mood Health | 60 Veg CapsFrom $13.99 $46.63Check Price on Shopee-78%Biofinest Probiotic 50 Billion CFU Enzyme Supplement 12 + 3 Prebiotics – Diet Slimming Eczema Detox Men Women (60 caps)From $22.40 $101.82Check Price on Shopee-28%Optimum Nutrition, Gold Standard, 100% Whey Protein Powder, 2lbs (907g ) / 5 lbs (2.27 kg) / 10 lbs (4.54 kg)From $42.04 $58.39Check Price on Shopee-52%Optimum Nutrition, Micronized Creatine Powder, Build Muscle, Workout Support, Unflavored, 300g-1200gFrom $32.88 $68.50Check Price on Shopee
OMY Liquid Hyaluron 2.0 | Marine Collagen 28,000mg + PDRN 1,000mg | Hydrating Bouncy Skin Glow Drink$70.00Check Price on Shopee-55%Biofinest Effervescent Vitamin C 1000mg D3 Zinc Collagen Multivitamin Calcium Magnesium Zinc Tablets Drink Sugar FreeFrom $5.35 $11.89Check Price on Shopee【 SG Stock 】All-In-One Multi Pouch Shake / Macadamia, Cinnamon, Chocolate / Protein, Korea Diet meal$9.90Check Price on Shopee-60%Estalife Daily Pre + Probiotics Melts + Enzyme | 15 Billion CFU + Inulin + Bromelain | 肠道保健From $19.99 $49.98Check Price on Shopee-70%Estalife Magnesium Glycinate 1000MG | Heart, Bone, Muscle, Sleep, Mood Health | 60 Veg CapsFrom $13.99 $46.63Check Price on Shopee-78%Biofinest Probiotic 50 Billion CFU Enzyme Supplement 12 + 3 Prebiotics – Diet Slimming Eczema Detox Men Women (60 caps)From $22.40 $101.82Check Price on Shopee-28%Optimum Nutrition, Gold Standard, 100% Whey Protein Powder, 2lbs (907g ) / 5 lbs (2.27 kg) / 10 lbs (4.54 kg)From $42.04 $58.39Check Price on Shopee-52%Optimum Nutrition, Micronized Creatine Powder, Build Muscle, Workout Support, Unflavored, 300g-1200gFrom $32.88 $68.50Check Price on ShopeeRisk Factors for Developing GDM
Several factors can increase the likelihood of developing gestational diabetes:
Advanced maternal age becomes a significant factor when women are over 35 years of age, as metabolic changes and insulin resistance tend to increase with age.
Elevated body mass index poses risks when BMI reaches ≥23kg/m² for Asian women or ≥25kg/m² generally, as excess weight contributes to insulin resistance that can worsen during pregnancy.
Family history of diabetes in parents or siblings indicates genetic predisposition that may manifest during the metabolic stress of pregnancy.
Related article: Diabetes Treatment in Singapore: Types, Risks
Previous pregnancy with GDM significantly increases the likelihood of recurrence in subsequent pregnancies, as the underlying tendency toward glucose intolerance often persists.
Previous delivery of a baby weighing more than 4kg suggests previous undiagnosed or poorly controlled glucose levels that led to fetal overgrowth.
History of unexplained stillbirth or poor obstetric outcomes may indicate previous unrecognized glucose intolerance that affected pregnancy outcomes.
Polycystic ovary syndrome (PCOS) creates hormonal imbalances that affect insulin sensitivity and glucose metabolism, increasing diabetes risk.
Certain ethnic backgrounds including Southeast Asian, Black, African-Caribbean, or Middle-Eastern origin carry higher genetic predisposition to insulin resistance and diabetes development.
It’s important to remember that GDM can develop in any pregnant woman, even without these risk factors, which is why routine screening is recommended for all pregnant women regardless of their individual risk profile.
You might like: Type 1 Diabetes Treatment in Singapore: Causes, Risks
Screening and Diagnosis for GDM in Singapore
In Singapore, screening for GDM is recommended for all pregnant women, typically between weeks 24 and 28 of pregnancy.
However, if you have risk factors, testing may be performed earlier and repeated later if the initial test is normal.
The standard screening method is the Oral Glucose Tolerance Test (OGTT):
How the OGTT Works
There are two types of glucose screening tests commonly used:
One-Step Testing:
- Requires fasting for 8 to 14 hours before the test (only sips of water allowed)
- Initial blood draw to measure fasting glucose levels
- Consumption of a 75-gram glucose solution
- Additional blood samples taken at one-hour and two-hour intervals
You might be interested: Type 2 Diabetes Treatment in Singapore: Symptoms, Risks
Two-Step Testing:
- First step does not require dietary changes; you simply fast overnight and have blood drawn after drinking a glucose solution
- If results indicate elevated glucose levels, a second 3-hour glucose tolerance test is conducted
- This second test requires 8-14 hours of fasting, followed by consumption of a 100-gram glucose solution
- Blood is drawn initially and then three more times over a 3-hour period
GDM is diagnosed if any of the following glucose readings are elevated:
- Fasting glucose level: ≥5.1mmol/L
- 1-hour post OGTT glucose level: ≥10.0mmol/L
- 2-hours post OGTT glucose level: ≥8.5mmol/L
Health Implications of Uncontrolled GDM
If gestational diabetes is not properly managed, it can lead to complications for both mother and baby.
Risks for the Mother:
- Preeclampsia: A serious complication causing high blood pressure that can threaten both the mother’s and baby’s life
- Increased likelihood of cesarean delivery due to baby’s size
- Higher risk of developing type 2 diabetes later in life
- Increased risk of GDM in future pregnancies
Risks for the Baby:
- Macrosomia: Excessive growth making the baby larger than average (>4kg), which can complicate delivery
- Hypoglycemia (low blood sugar) after birth, potentially causing seizures if untreated
- Respiratory distress syndrome due to underdeveloped lungs
- Jaundice (yellowing of the skin and eyes)
- Higher risk of obesity and type 2 diabetes later in life
- In rare cases, increased risk of stillbirth
Read more: Diabetes Myths Debunked: Separating Fact from Fiction
Managing Gestational Diabetes in Singapore
The good news is that with proper management, most women with GDM have normal pregnancies and healthy babies. Treatment focuses on controlling blood glucose levels through a multi-faceted approach:
1. Blood Sugar Monitoring

Regular monitoring of blood glucose levels is essential for managing GDM and requires active participation from expectant mothers.
You’ll be taught how to use a glucose monitoring device for home testing, ensuring you can accurately track your levels throughout the day.
Typical monitoring schedule includes checking levels before and 2 hours after each meal, and before bedtime, providing comprehensive data about how your body responds to food and daily activities.
Your healthcare provider will establish target glucose ranges specifically tailored for you and your pregnancy needs.
Keeping a record of your readings to share with your healthcare team allows for ongoing assessment and treatment adjustments as needed.
Related article: Pituitary Gland Disorders Treatment in Singapore: Symptoms, Causes
2. Nutritional Management and Dietary Plan
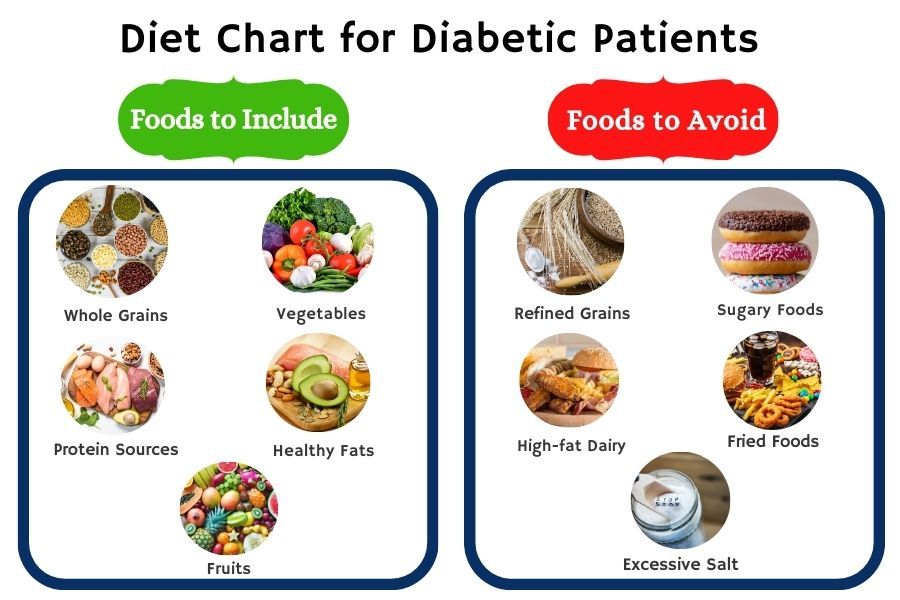
Diet plays a crucial role in controlling GDM. In Singapore, you’ll likely be referred to a dietitian who will create a personalized meal plan based on your needs. General dietary recommendations include:
Carbohydrates (45% of daily calorie intake)
Carbohydrate management forms the foundation of dietary control for gestational diabetes.
Focusing on complex carbohydrates that release glucose slowly helps prevent dangerous blood sugar spikes throughout the day.
Distributing carbohydrate intake throughout the day with 3 meals and 2-4 snacks ensures steady energy levels and better glucose control.
Choosing high-fiber options like brown rice, whole grains, oats, quinoa, and legumes provides sustained energy while supporting digestive health.
Avoiding processed foods with added sugars and sugary beverages prevents rapid glucose elevation that can be harmful during pregnancy.
You might like: Cushing Syndrome Treatment: Causes, Symptoms
Proteins (20-25% of daily calorie intake)
Adequate protein intake supports both maternal health and fetal development.
Including quality protein sources like eggs, lean meats, fish, tofu, and legumes ensures you receive essential amino acids needed during pregnancy.
Protein helps stabilize blood sugar levels while simultaneously supporting your baby’s crucial development, particularly brain and organ formation.
Healthy Fats (25-30% of daily calorie intake)
Essential fatty acids play a vital role in fetal brain development and maternal health.
Including sources of essential fatty acids needed for optimal brain development ensures your baby receives crucial nutrients for neurological growth.
Incorporating avocados, unsalted nuts, seeds, and healthy oils such as olive and canola oil provides beneficial fats without excess saturated fat.
Limiting saturated and trans fats protects both maternal cardiovascular health and supports optimal pregnancy outcomes.
Foods to Specifically Avoid
Certain foods pose particular risks during pregnancy with gestational diabetes.
Alcoholic drinks should be completely eliminated as they pose risks to fetal development and can affect blood sugar control.
Processed foods with added sugar cause rapid blood glucose spikes that are difficult to manage during pregnancy. Sweet pastries and desserts provide empty calories and dangerous glucose elevation without nutritional benefits.
Sugary drinks including fruit juices, sodas, and sweetened beverages deliver concentrated sugars that overwhelm the body’s glucose management systems.
Foods high in simple carbohydrates that cause blood sugar spikes should be avoided as they make glucose control extremely challenging.
3. Physical Activity
Regular exercise plays an important role in managing GDM by improving insulin sensitivity and glucose utilization.
Aiming for at least 150 minutes of moderate-intensity physical activity per week provides optimal benefits for glucose control and overall pregnancy health.
Walking is an excellent, safe option for pregnant women as it requires no special equipment and can be easily incorporated into daily routines.
Swimming can also be beneficial as it provides low-impact exercise that’s gentle on joints while supporting the growing belly.
Always consulting with your healthcare provider before starting any exercise program ensures that your specific pregnancy circumstances are considered and that activities are appropriate for your condition.
4. Medication When Necessary
When diet and exercise alone cannot adequately control blood glucose levels, medical intervention becomes necessary to protect both mother and baby.
Oral medication (metformin) may be prescribed as a first-line treatment when lifestyle modifications prove insufficient.
Insulin injections may be necessary in some cases where oral medications are inadequate or contraindicated during pregnancy.
Medication is typically only needed during pregnancy and is discontinued after delivery once hormone levels return to normal.
Your healthcare team will provide detailed instructions on proper administration techniques, timing, and monitoring to ensure safe and effective treatment.
5. Mental Well-being Support
Being diagnosed with GDM can cause significant anxiety and stress for expectant mothers, making emotional support an essential component of comprehensive care.
Sharing your concerns with your healthcare team ensures you receive professional guidance and reassurance about your condition and treatment.
Remembering that GDM is not your fault helps reduce feelings of guilt or self-blame that many women experience after diagnosis.
Connecting with support groups of women experiencing similar challenges provides valuable peer support and practical advice from others who understand your experience.
Practicing stress-reduction techniques like gentle yoga, meditation, or deep breathing exercises helps manage anxiety while potentially improving glucose control.
Focusing on the positive steps you’re taking to ensure your and your baby’s health reinforces your active role in achieving the best possible outcomes.
Delivery and Post-Pregnancy Care
During Delivery:
- Your healthcare team will monitor your blood glucose levels during labor
- If necessary, insulin may be administered intravenously
- Your baby’s glucose levels will be monitored after birth
After Delivery:
- For most women, blood glucose levels return to normal shortly after delivery
- A follow-up OGTT is recommended 6-12 weeks postpartum to confirm GDM has resolved
- Your baby may require monitoring for hypoglycemia initially
Long-term Follow-up:
- Women who have had GDM have a higher lifetime risk of developing type 2 diabetes
- Annual or regular diabetes screening is recommended
- Maintaining a healthy lifestyle with proper nutrition and regular exercise can reduce this risk
- Inform your doctor about your history of GDM before future pregnancies
Specialized Care in Singapore
Singapore offers comprehensive care for women with GDM, including:
- Specialized antenatal clinics for women with GDM
- Multidisciplinary teams including obstetricians, endocrinologists, dietitians, and diabetes nurse educators
- Access to advanced monitoring and treatment options
- Postnatal follow-up care
- Support services for lifestyle modifications
FAQ on Gestational Diabetes in Singapore
What exactly is gestational diabetes?
Gestational diabetes mellitus (GDM) is a type of diabetes that develops only during pregnancy, typically in the second or third trimester. It occurs when your body cannot produce enough insulin or use insulin effectively to manage blood sugar levels during pregnancy.
This condition is caused by hormonal changes that affect how your body processes glucose.
Unlike other types of diabetes, GDM usually resolves after delivery, though it increases your risk of developing type 2 diabetes later in life.
How common is gestational diabetes in Singapore?
In Singapore, gestational diabetes affects approximately one in five pregnant women (20%), which is notably higher than global averages.
This high prevalence may be related to the ethnic composition of Singapore’s population, as women of Asian descent have a genetically higher risk of developing GDM compared to other ethnicities.
Why do I need to be screened for GDM?
Screening is essential because GDM often has no noticeable symptoms, yet it can cause significant complications if left unmanaged.
Early detection allows for timely intervention, significantly reducing risks for both mother and baby.
All pregnant women in Singapore are recommended to undergo GDM screening, regardless of risk factors, as the condition can develop in any pregnancy.
When is GDM screening performed in Singapore?
In Singapore, routine screening for GDM typically occurs between weeks 24 and 28 of pregnancy.
However, if you have risk factors such as previous GDM, family history of diabetes, or a BMI over 23 kg/m², your doctor may recommend earlier screening, sometimes as early as the first trimester, with repeat testing later if the initial results are normal.
How do I prepare for the oral glucose tolerance test?
To prepare for the OGTT, you should:
- Fast for 8-14 hours before the test (usually overnight)
- You may drink small sips of water during the fasting period
- Avoid smoking before the test
- Inform your doctor about any medications you’re taking
- Continue your normal diet in the days leading up to the test
- Allow approximately 2-3 hours for the entire testing procedure
Will I need insulin or medication for my gestational diabetes?
Not all women with GDM require medication.
Approximately 70-85% of women with GDM in Singapore can manage their condition through dietary changes and regular physical activity alone.
Medication (either oral metformin or insulin injections) is typically only prescribed when blood glucose targets cannot be met with lifestyle modifications.
Your healthcare team will regularly review your blood glucose readings to determine if medication is necessary.
How will gestational diabetes affect my delivery?
Having well-controlled GDM does not necessarily change your delivery plans.
However, your healthcare provider will monitor your pregnancy more closely, including regular growth scans to check your baby’s size.
If your baby is measuring large (macrosomia) or there are other concerns, your doctor might recommend inducing labor or scheduling a cesarean section.
Additionally, your blood glucose levels will be monitored during labor to ensure they remain within the target range.
Will my baby need special care after birth?
Babies born to mothers with GDM may require some additional monitoring after birth.
Healthcare providers will check your baby’s blood glucose levels shortly after delivery to ensure they’re not developing hypoglycemia (low blood sugar).
Most babies require only temporary monitoring, but if your baby’s glucose levels are low, they may need feeding sooner or, in some cases, receive glucose solution.
Your baby will also be monitored for other potential complications like jaundice or respiratory issues.
Can I breastfeed if I had gestational diabetes?
Not only can you breastfeed, but it’s highly encouraged!
Breastfeeding provides numerous benefits for both mother and baby.
For mothers who had GDM, breastfeeding can help lower blood glucose levels, promote weight loss, and reduce the risk of developing type 2 diabetes in the future.
For babies, breast milk provides optimal nutrition and may help reduce their future risk of developing obesity and diabetes.
What follow-up care will I need after pregnancy?
After delivery, you should have a follow-up OGTT at 6-12 weeks postpartum to confirm that your blood glucose levels have returned to normal.
Even if this test is normal, women who had GDM should have annual diabetes screenings for at least three years, as the risk of developing type 2 diabetes is significantly higher.
Your healthcare provider may also recommend regular check-ups to monitor other health parameters like blood pressure and cholesterol levels.
What can I do to prevent type 2 diabetes after having GDM?
To reduce your risk of developing type 2 diabetes after having GDM:
- Maintain a healthy weight through balanced nutrition
- Engage in regular physical activity (aim for at least 150 minutes per week)
- Attend all recommended follow-up appointments and screenings
- Breastfeed your baby if possible
- Limit intake of refined carbohydrates and sugary foods
- Get adequate sleep
- Manage stress effectively
- Consider meeting with a dietitian for personalized nutritional advice
What are the chances of developing GDM in future pregnancies?
Women who have had GDM have a 30-50% chance of developing it again in subsequent pregnancies.
This risk can be somewhat reduced by maintaining a healthy weight between pregnancies, following a balanced diet, and staying physically active.
If you’re planning another pregnancy after having GDM, it’s advisable to discuss this with your healthcare provider beforehand, as they may recommend early screening and additional monitoring during your next pregnancy.
Are there any support groups for women with GDM in Singapore?
Yes, there are several support resources available in Singapore for women with GDM.
Many hospitals and polyclinics offer support groups and educational programs specifically for women with GDM.
Additionally, organizations like the Diabetes Society of Singapore provide resources and community support.
Your healthcare provider can connect you with appropriate support groups, or you can explore online communities where women share experiences and advice about managing GDM.
Shortcutx Max Fat Burner Juice • Made in UK • Weight Loss Supplement for Slimming • Clinically proven (7 sachets)From $39.00Check Price on ShopeeOptimum Nutrition Gold Standard 100% Whey Protein, 5 LBs | Double Rich Chocolate | Primary Source Isolate$139.40Check Price on Shopee-13%Tradishot Detox Juice • Traditional Modern Tasty Jamu • Natural Herbal Supplement • Tumeric shot [7 x 35ml]From $24.36 $28.00Check Price on Shopee-18%Tradishot Immunity Boost Drink | Turmeric Shot (Extra Strength) | Boost Immunity Energy & Well-being [7x35mL]$24.60 $30.00Check Price on Shopee-55%Biofinest Gummy Vitamin Supplement – Beauty Energy Sleep Metabolism Men Women Kids Probiotics Multivitamin (60 Gummies)From $17.95 $39.89Check Price on Shopee-75%I Love Smart Heart Goat Pet Milk 70ml 400ml for Cats and DogsFrom $1.26 $5.04Check Price on Shopee[NEW] Shortcutx Max+ Advanced Fat Burner Juice • Improved Formula For Extreme Weight Loss (15x35ml)$81.90Check Price on Shopee-65%PM12 Balporo Bbae 1Box [Slimming, Weight Loss supplement, Garcinia,Vitamin, Effervescent]From $12.39 $35.40Check Price on Shopee