
What is Age-Related Macular Degeneration?
Age-Related Macular Degeneration (AMD) is a progressive eye condition that affects the macula, the central part of the retina responsible for sharp, central vision.
As one of the leading causes of vision impairment among people aged 50 and above in Singapore, AMD results in the deterioration of central vision while peripheral vision typically remains intact.
The retina functions similarly to film in a camera – capturing images through photoreceptor cells that convert visual information into nerve signals sent to the brain.
The macula, being the central portion of this retina, enables us to see fine details, differentiate colors, and perform daily activities like reading, recognizing faces, and driving.
When AMD develops, the central vision gradually deteriorates, making these everyday tasks challenging while still allowing for mobility and independence through preserved peripheral vision.
Read more: Which Eye Clinic in Singapore Should You Consider? (Sort by Reviews)
Types of Age-Related Macular Degeneration
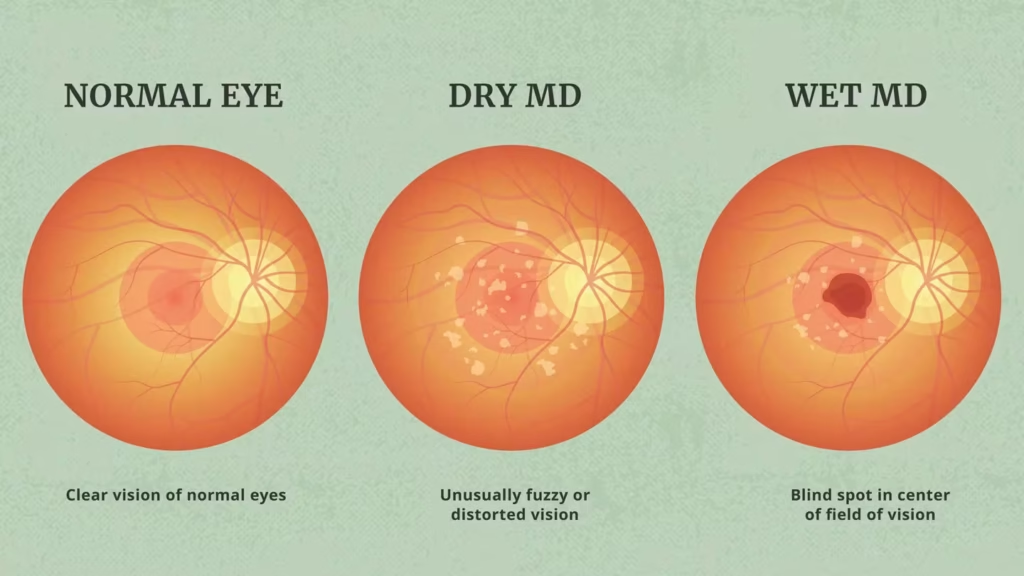
AMD manifests in two primary forms:
Dry AMD (Atrophic)
Dry AMD accounts for approximately 90% of all AMD cases. It develops as the light-sensitive cells in the macula slowly break down with age, leading to a gradual loss of central vision.
The hallmark of dry AMD is the presence of drusen – yellowish deposits that accumulate under the retina.
While most people with drusen don’t experience vision loss initially, as these deposits grow in size and number, they may lead to:
- Thinning of the light-sensitive layer in the macula
- Geographic atrophy (tissue death in advanced stages)
- Formation of blind spots in central vision
Progression of dry AMD typically occurs slowly over years, allowing patients to adapt gradually to vision changes.
You might be interested: The Ultimate Guide to Treating Dry Eyes in Singapore
Wet AMD (Exudative or Neovascular)
Wet AMD is less common but more aggressive, accounting for around 10% of cases while causing approximately 90% of severe vision loss from AMD.
It typically develops from pre-existing dry AMD and is characterized by:
- Growth of abnormal blood vessels (choroidal neovascularization) under the retina
- Leakage of blood, fluid, lipids, and proteins from these vessels
- Disruption of normal retinal structure
- Formation of scar tissue, often resulting in permanent vision loss if left untreated
The “wet” form can cause rapid deterioration of vision over days or weeks, making prompt diagnosis and treatment crucial.
A variant of wet AMD common in Asian populations, including Singaporeans, is polypoidal choroidal vasculopathy (PCV), affecting approximately 40-50% of wet AMD cases in Asia.
This subtype presents with grape-like abnormal vessels that can cause extensive bleeding and scarring.
Related article: Glaucoma in Singapore: Prevention and Treatment
Symptoms of Age-Related Macular Degeneration
Early AMD often produces mild or no symptoms. As the condition progresses, individuals may experience:
- Blurring of central vision (gradual in dry AMD, often rapid in wet AMD)
- Shadows or missing areas in the visual field
- Distorted vision (straight lines appearing wavy)
- Difficulty distinguishing colors, especially similar shades
- Reduced contrast sensitivity (difficulty telling different brightness levels apart)
- Slow recovery of visual function after exposure to bright light
- Need for brighter lighting for reading or close-up work
An important early warning sign of wet AMD is metamorphopsia—where straight lines appear wavy or distorted.
This can be detected using an Amsler grid test, a simple screening tool that patients can use at home.
You might like: The Ultimate Guide to Managing Myopia in Singapore
Risk Factors for Age-Related Macular Degeneration
Several factors increase the risk of developing AMD:
Non-Modifiable Risk Factors:
- Age: Risk increases significantly with age. A 1997 study showed that one in four Singaporeans aged 60 and above had this condition. By age 75, approximately 1 in 3 people will have some form of AMD.
- Family history: Genetic predisposition plays a significant role.
- Light eye color: People with lighter iris color may be at higher risk.
- Light skin tone: Fair-skinned individuals appear more susceptible.
Modifiable Risk Factors:
- Smoking: Smokers are more than four times likely to develop wet AMD than non-smokers.
- Obesity: Maintaining a healthy weight reduces risk.
- Cardiovascular diseases: Conditions affecting heart health also impact eye health.
- High blood pressure: Hypertension increases risk.
- High cholesterol: Lipid management is important for eye health.
- Poor diet: Low intake of antioxidants and high fat consumption increases risk.
- Excessive sunlight exposure: UV radiation may contribute to AMD development.
You might be interested: The Ultimate Guide to Ptosis Treatment in Singapore
Diagnosis of Age-Related Macular Degeneration
Early diagnosis is crucial for effective management of AMD. A comprehensive dilated eye examination by an ophthalmologist may include:
Amsler Grid Test
This simple screening tool helps detect changes in central vision. Patients focus on a central dot within a grid pattern.
If lines appear wavy, fuzzy, or if certain sections are missing, AMD may be present. This test can also be performed at home for regular monitoring.
Fundus Fluorescein Angiogram (FFA) and Indocyanine Green Angiogram (ICG)
These tests involve injecting a fluorescent dye into a vein in the arm.
The dye circulates through blood vessels in the eye, allowing photographs to highlight abnormal or leaking vessels characteristic of wet AMD.
Though uncommon, some patients may experience nausea or rare allergic reactions to the dye.
Related article: Understanding Corneal Ulcers: Prevention, Causes, and Treatment Options
Optical Coherence Tomography (OCT)
OCT uses light waves to capture detailed cross-sectional images of the retina, similar to an ultrasound but with higher resolution.
This non-invasive, radiation-free imaging technique provides detailed visualization of retinal layers and helps detect fluid or structural changes.
Optical Coherence Tomography Angiography (OCT-A)
Based on the same technology as OCT, this newer technique allows examination of blood vessels without requiring dye injection, making it safer and more convenient for patients needing frequent monitoring.
Related article: Managing Your Child’s Myopia: Prevention and Treatment Options
Prevention of Age-Related Macular Degeneration
While there’s no foolproof method to prevent AMD, several strategies may reduce risk and slow progression:
Lifestyle Modifications
- Quit smoking: One of the most significant modifiable risk factors.
- Maintain a healthy diet: Consume foods rich in:
- Leafy green vegetables
- Colorful fruits and vegetables
- Oily fish (high in omega-3 fatty acids)
- Reduced fat intake
- Regular exercise: Helps maintain healthy weight and improves circulation.
- Protect eyes from UV light: Wear quality sunglasses or brimmed hats outdoors.
- Control cardiovascular risk factors: Manage blood pressure, cholesterol levels, and weight.
Nutritional Supplements
The AREDS2 (Age-Related Eye Disease Study 2) formulation of vitamins and minerals has been shown to reduce the risk of advanced AMD progression by about 25% over 5 years in high-risk patients.
However, these supplements are not beneficial for everyone. It’s essential to consult an ophthalmologist to determine if supplements would be appropriate for your specific situation.
Regular Eye Examinations
Early detection through regular comprehensive eye examinations is crucial, especially for individuals over 50 or those with known risk factors.
Early diagnosis significantly improves treatment outcomes, particularly for wet AMD.
Home Monitoring
Self-monitoring using tools like the Amsler grid can help detect subtle vision changes between professional examinations.
Patients can also use everyday objects with straight lines (like bathroom tiles or window panes) as informal monitoring tools.
Treatment Options for Age-Related Macular Degeneration
Treatment approaches differ based on the type and stage of AMD:
Dry AMD Management
Currently, there is no known treatment that can reverse dry AMD. Management focuses on:
- Nutritional supplements: The AREDS2 formulation may slow progression in certain patients.
- Lifestyle modifications: As outlined in prevention strategies.
- Regular monitoring: To detect conversion to wet AMD, which requires immediate treatment.
- Low vision aids: For those with significant vision loss.
Research continues on potential treatments, including:
- Brimonidine eye drops, which have shown success in slowing optic nerve degeneration in glaucoma
- Retinal stem cell therapy, which may eventually replace atrophic tissue
Wet AMD Treatment
Intravitreal Injections
The mainstay of wet AMD treatment involves anti-vascular endothelial growth factor (anti-VEGF) medications injected directly into the eye.
These drugs block the growth of abnormal blood vessels. Options include:
- Bevacizumab (Avastin)*
- Ranibizumab (Lucentis)
- Aflibercept (Eylea)
- Brolucizumab (Beovu)
*Use of Avastin for eye treatment is off-label but is safely used in all public hospitals and institutions in Singapore.
The treatment protocol typically involves:
- A loading phase of monthly injections for the first three months
- A maintenance phase where treatment intervals may be extended based on disease activity (“treat and extend” approach)
The injection procedure is performed after numbing the eye with anesthetic drops. Most patients feel pressure but minimal pain.
On average, patients require 8 injections in the first year, decreasing to 3-5 injections annually in subsequent years. Some may need ongoing treatment for life.
Treatment outcomes are encouraging:
- Over 90% of treated patients avoid significant vision loss
- 70% maintain their current vision level
- Approximately 40% experience significant vision improvement
- About 50% retain vision sufficient for driving (6/12 or better)
Photodynamic Therapy (PDT)
Also known as “cold laser” treatment, PDT involves:
- Injecting a light-sensitive drug (verteporfin/Visudyne) into the bloodstream
- Activating the drug with a “cold” laser when it reaches abnormal blood vessels
- Sealing leaking vessels without damaging surrounding tissue
PDT is particularly effective when combined with anti-VEGF therapy for treating polypoidal choroidal vasculopathy (PCV), the Asian variant of wet AMD.
Laser Photocoagulation
In select cases, thermal “hot” laser may be used to seal abnormal blood vessels. However, this approach has largely been replaced by newer treatments.
Emerging Treatments
Several promising treatments are in development:
- Port delivery system: An implantable device that can store and slowly release medication, requiring less frequent refills
- Abicipar: A longer-acting anti-VEGF injection lasting up to 12 weeks
- RGX-314: A gene therapy approach potentially blocking VEGF for years after a single surgical procedure
Living with Age-Related Macular Degeneration
Despite vision loss, most AMD patients maintain sufficient peripheral vision to lead independent lives. Several approaches can help manage daily activities:
Low Vision Aids
Various assistive devices can help maximize remaining vision:
- Magnifiers for near and distance vision
- Desktop and handheld magnifying glasses
- Telescopes
- Electronic magnifiers
- Computer screen readers
- High-contrast clocks, phones, and other devices
Adaptive Strategies
- Increased lighting for reading and close work
- High-contrast materials (black text on white background)
- Large-print books and publications
- Voice command technology
- Text-to-speech software
Psychological Support
Adjusting to vision changes can be emotionally challenging.
Support groups, counseling, and connecting with others experiencing similar challenges can provide valuable emotional assistance.
Regular Monitoring
Ongoing monitoring is essential for:
- Tracking disease progression
- Detecting conversion from dry to wet AMD
- Assessing treatment effectiveness
- Adjusting management strategies as needed
AMD in Singapore: Local Context
Singapore faces a significant AMD burden due to its rapidly aging population. According to local research:
- Approximately one in four Singaporeans aged 60 and above have AMD
- The condition is one of the top three causes of blindness in Singapore
- For those aged 60 and above, the incidence is 12.5%, increasing to 33% by age 80
- Studies from the Singapore Eye Research Institute confirm that smokers are four times more likely to develop wet AMD than non-smokers
Local healthcare institutions offer comprehensive AMD management with access to the latest diagnostic tools and treatment options.
Research into AMD continues through institutions like the Singapore Eye Research Institute, which conducts clinical trials evaluating new treatments specifically for Asian populations.
Conclusion
Age-related macular degeneration represents a significant health challenge, particularly in Singapore’s aging society.
While it can cause serious vision impairment, early detection, appropriate treatment, and adaptive strategies can help maintain quality of life.
Understanding risk factors, recognizing symptoms, and seeking prompt medical attention are crucial steps in managing this condition.
Ongoing research continues to improve treatment options, particularly for wet AMD, offering hope for better outcomes in the future.
For those already affected, numerous resources and support systems exist to help navigate life with AMD while maintaining independence and quality of life.
Frequently Asked Questions
What is the difference between dry and wet AMD?
Dry AMD accounts for 90% of cases and involves the gradual breakdown of light-sensitive cells in the macula, resulting in slow, progressive vision loss.
Wet AMD, though less common at 10% of cases, is more aggressive and caused by abnormal blood vessel growth under the retina.
These vessels leak fluid and blood, often leading to rapid vision deterioration and accounting for 90% of severe AMD-related vision loss.
Can AMD cause complete blindness?
AMD rarely causes complete blindness. The condition primarily affects central vision, which we use for activities like reading, recognizing faces, and driving.
Peripheral (side) vision typically remains intact, allowing most people to maintain independence with many daily activities.
While legally classified as “blindness,” individuals with advanced AMD usually retain navigational vision.
How effective are anti-VEGF injections for wet AMD?
Anti-VEGF injections are highly effective for wet AMD when started promptly.
Clinical outcomes show that over 90% of treated patients avoid significant vision loss, 70% maintain their current vision, and approximately 40% experience meaningful vision improvement.
About 50% retain vision good enough for driving (6/12 or better). Results vary based on how early treatment begins and individual response.
How many injections will I need for wet AMD treatment?
The number of injections varies by individual and disease severity. On average, patients require up to 8 injections in the first year of treatment.
The frequency typically decreases to 3-5 injections annually in subsequent years.
Some patients may need ongoing treatment for life, while others experience extended periods of disease inactivity requiring fewer injections.
Are there any side effects from intravitreal injections?
Most patients tolerate intravitreal injections well, experiencing only mild discomfort during the procedure.
Possible side effects include temporary pressure sensation, slight burning from antiseptic solution, and occasionally small surface bleeding at the injection site.
Serious complications are rare but may include eye infection (endophthalmitis), inflammation, vitreous hemorrhage (bleeding into the eye’s gel), or retinal detachment.
What dietary changes can help with AMD?
A diet beneficial for AMD management includes foods rich in antioxidants and omega-3 fatty acids.
This means increasing consumption of leafy green vegetables (spinach, kale), colorful fruits and vegetables (rich in carotenoids), and oily fish (salmon, mackerel).
Reducing intake of saturated fats and processed foods is also recommended. These dietary patterns help provide nutrients that support macular health.
How is AMD different in Asian populations compared to Western populations?
AMD in Asian populations often presents differently than in Western populations.
A significant difference is the higher prevalence (40-50%) of polypoidal choroidal vasculopathy (PCV) in Asian wet AMD cases.
This variant has grape-like abnormal vessels that can cause extensive bleeding. Treatment approaches may vary, with combination therapy of anti-VEGF injections and photodynamic therapy often being more effective for Asian patients with PCV.
Can the AREDS2 supplements prevent AMD?
AREDS2 supplements are not designed to prevent AMD development but rather to slow progression in people already diagnosed with intermediate or advanced AMD.
Studies show these supplements reduce the risk of progression to advanced AMD by about 25% over 5 years, but only in specific high-risk patients.
They are not recommended for everyone and should only be taken under an ophthalmologist’s guidance.
How often should I get my eyes checked for AMD risk?
Adults with no symptoms or risk factors should have comprehensive eye exams every 1-2 years after age 50.
Those with AMD risk factors (family history, smoking history, etc.) should be examined annually.
Patients already diagnosed with early AMD should follow their ophthalmologist’s recommendation, typically every 6-12 months.
Those with intermediate or advanced AMD may need examinations every 3-6 months.
What new treatments for AMD are being developed?
Several promising treatments are in development, including: longer-lasting anti-VEGF medications requiring fewer injections; port delivery systems (implantable reservoirs that slowly release medication);
gene therapy approaches like RGX-314 that could potentially block VEGF for years after a single procedure; and stem cell therapies that might replace damaged retinal tissue.
For dry AMD, treatments targeting inflammation and complement pathways are being investigated.